The practice of allowing pharmaceutical companies to advertise directly to consumers began in the United States in 1997, following a significant shift in regulatory policy by the Food and Drug Administration (FDA). Prior to this, pharmaceutical advertising was primarily targeted at healthcare professionals, but a relaxation of guidelines under the FDA’s *Changes to Prescription Drug Advertising Regulations* permitted companies to market prescription medications directly to the public through television, print, and other media. This move marked a turning point in the industry, sparking debates about the ethical implications, the impact on healthcare costs, and the influence of such advertising on patient-doctor relationships. The U.S. remains one of the few countries globally where direct-to-consumer pharmaceutical advertising is legal, setting it apart from most other nations with stricter regulations.
| Characteristics | Values |
|---|---|
| Year Direct-to-Consumer (DTC) Advertising Began in the U.S. | 1983 (Initial allowance, but later paused) |
| Year DTC Advertising Fully Legalized in the U.S. | 1997 (FDA relaxed restrictions, leading to widespread DTC advertising) |
| Key Regulation Change | FDA's 1997 guidance on consumer-directed broadcast ads for prescription drugs |
| First Major DTC Ad Campaign | 1997 - Merck's "Claritin" campaign |
| Countries Allowing DTC Advertising | Primarily the U.S. and New Zealand (with strict regulations) |
| Impact on Prescription Drug Sales | Significant increase in consumer requests for advertised medications |
| Criticisms | Over-prescription, high costs, and potential for misleading information |
| Latest Trends | Increased scrutiny and calls for regulation or bans in the U.S. |
Explore related products



$228.97 $242



What You'll Learn
- s Policy Shift: Deregulation allowed direct-to-consumer pharmaceutical advertising to begin in the United States
- FDA Role: The FDA relaxed rules in 1997, enabling broader TV and print drug ads
- Global Variations: Most countries still ban direct-to-consumer pharmaceutical advertising, unlike the U.S
- Industry Impact: Advertising boosted drug sales and patient requests for specific medications significantly
- Ethical Concerns: Critics argue ads prioritize profits over public health and medical necessity
![]()
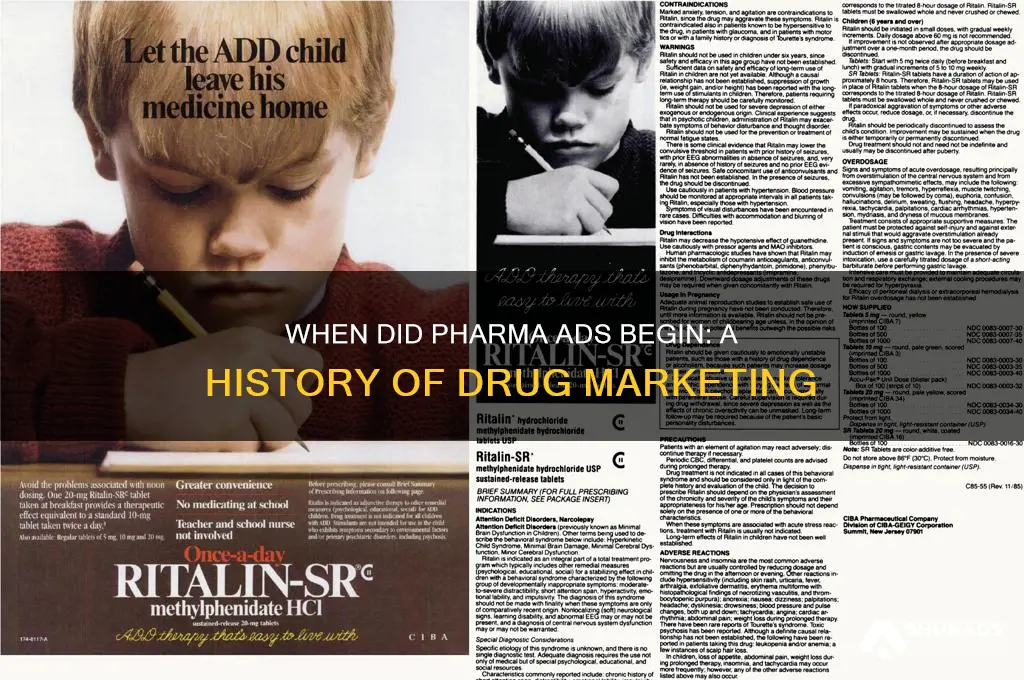
1980s Policy Shift: Deregulation allowed direct-to-consumer pharmaceutical advertising to begin in the United States
The 1980s marked a pivotal shift in the pharmaceutical landscape when the United States began allowing direct-to-consumer (DTC) advertising. This deregulation, spearheaded by the Food and Drug Administration (FDA), permitted drug companies to market prescription medications directly to the public for the first time. Prior to this, pharmaceutical promotions were limited to medical professionals, but the new policy opened the floodgates for TV, print, and radio ads targeting everyday consumers. This change was driven by the belief that informed patients would take a more active role in their healthcare, potentially leading to better health outcomes. However, it also raised concerns about over-medicalization and the potential for misleading information.
Analyzing the impact of this policy shift reveals both benefits and drawbacks. On one hand, DTC advertising increased public awareness of medical conditions and available treatments. For instance, campaigns for cholesterol-lowering statins like Lipitor in the late 1990s educated millions about the risks of heart disease. This led to earlier diagnoses and proactive management of chronic conditions. On the other hand, critics argue that such ads often oversimplify complex medical issues, emphasizing benefits while downplaying risks. A 2004 study found that 30% of DTC ads lacked balanced information about side effects, potentially leading to inappropriate medication use. For example, ads for antidepressants like Paxil often highlighted mood improvement without adequately addressing withdrawal symptoms or dependency risks.
Instructively, understanding how to critically evaluate DTC ads is essential for consumers. Start by noting the medication’s generic name, not just the brand, to research it independently. Pay attention to the fine print or voiceover disclaimers, which often list side effects and contraindications. For instance, ads for blood thinners like Eliquis may mention bleeding risks in small text. Cross-reference the information with trusted sources like the FDA or Mayo Clinic. If an ad prompts you to ask your doctor about a medication, prepare specific questions: “Is this drug necessary for my condition?” or “Are there non-pharmaceutical alternatives?” This proactive approach ensures informed decision-making rather than blind reliance on marketing.
Comparatively, the U.S. stands out as one of the few countries allowing DTC pharmaceutical advertising. Nations like Canada and the European Union maintain stricter regulations, limiting promotions to healthcare providers. A 2017 study comparing U.S. and Canadian prescription rates found that Americans were 50% more likely to request advertised medications, often for conditions like erectile dysfunction or anxiety. While this highlights the effectiveness of DTC ads in driving sales, it also underscores the potential for overprescription. For example, ads for ADHD medications like Adderall have been criticized for contributing to a 42% increase in diagnoses among adults between 2007 and 2016, raising questions about whether all cases were clinically justified.
Descriptively, the evolution of DTC advertising reflects broader societal trends. The 1980s deregulation coincided with the rise of consumerism in healthcare, where patients began demanding more control over their treatment options. Early ads were straightforward, often featuring a doctor explaining the drug’s benefits. By the 2000s, campaigns became more sophisticated, incorporating emotional storytelling and celebrity endorsements. For instance, Sally Field’s 2008 ad for Boniva osteoporosis medication resonated with middle-aged women by framing the drug as a way to stay active and independent. Today, digital platforms like social media and targeted online ads further personalize marketing, though they also raise privacy concerns. This ongoing adaptation highlights the enduring influence of the 1980s policy shift, shaping how pharmaceuticals are perceived and consumed in the U.S.
Mastering Treasury Analysis in Private Advertising: Strategies for Success
You may want to see also
Explore related products





![]()
FDA Role: The FDA relaxed rules in 1997, enabling broader TV and print drug ads
In 1997, the FDA’s decision to relax advertising rules marked a turning point for pharmaceutical marketing. Prior to this, drug companies were limited to providing detailed product information in lengthy, often confusing "brief summary" ads. The new regulations allowed for "product claim" ads, which could highlight a drug’s benefits without including the full list of risks in the initial presentation. This shift opened the floodgates for direct-to-consumer (DTC) advertising on television and in print, transforming how Americans learn about prescription medications.
Consider the practical implications of this change. Before 1997, a TV ad for a cholesterol-lowering drug might have been a 60-second monologue listing every potential side effect, from headaches to liver damage. Post-1997, the same ad could focus on a smiling, active senior enjoying life, with a voiceover briefly mentioning "possible side effects" and directing viewers to a website or toll-free number for details. This approach made ads more engaging but also raised concerns about oversimplification of risks. For instance, a statin ad might emphasize its ability to reduce LDL cholesterol by 30% without immediately clarifying that it’s intended for adults over 40 with a history of cardiovascular disease, not for everyone with mildly elevated cholesterol.
The FDA’s relaxed rules also spurred a surge in consumer awareness—and demand. By 2000, DTC spending had quadrupled to $2.5 billion annually, with ads for allergy medications, antidepressants, and erectile dysfunction drugs dominating airwaves. This had unintended consequences. Patients began requesting specific drugs by name, sometimes without fully understanding their medical necessity. For example, a patient might ask their doctor for a branded sleep aid after seeing an ad, even if a lifestyle change or over-the-counter remedy would suffice. Physicians reported feeling pressured to prescribe advertised drugs, even when cheaper generics were equally effective.
From a regulatory standpoint, the 1997 shift required a delicate balance. The FDA mandated that ads include a "major statement" of risks, but allowed flexibility in how and when this information was presented. For print ads, this often meant a small-print disclaimer at the bottom of the page. For TV, it translated to a rapid-fire voiceover at the end of the ad, a practice critics dubbed "fine-print on fast-forward." To navigate this, consumers were advised to treat ads as starting points, not endpoints. Practical tips included jotting down the drug’s generic name (e.g., sertraline for Zoloft) and researching it independently, or asking pharmacists to explain potential interactions with current medications.
In retrospect, the FDA’s 1997 decision democratized access to medical information but also introduced complexities. While DTC ads empowered patients to take an active role in their health, they also blurred the line between education and promotion. For instance, an ad for a migraine medication might highlight its efficacy in reducing attack frequency but omit that it’s only approved for adults 18–65 with a specific migraine subtype. Moving forward, consumers must approach these ads critically, using them as tools for informed conversations with healthcare providers rather than as prescriptions in themselves.
Should You Trust Companies That Still Fax Advertisements?
You may want to see also
Explore related products






![]()
Global Variations: Most countries still ban direct-to-consumer pharmaceutical advertising, unlike the U.S
The United States stands as a global outlier in permitting direct-to-consumer (DTC) pharmaceutical advertising, a practice that began in the early 1980s and was fully legalized in 1997. This contrasts sharply with most other countries, where such advertising remains banned or heavily restricted. For instance, the European Union, Canada, and Australia prohibit DTC ads, prioritizing physician-patient relationships and minimizing the risk of overmedication. This divergence raises questions about the impact of such advertising on healthcare systems, patient behavior, and public health outcomes.
Analyzing the rationale behind these global bans reveals a focus on patient safety and informed decision-making. In countries like the UK, where pharmaceutical ads are limited to healthcare professionals, the emphasis is on evidence-based prescribing rather than consumer demand. Studies suggest that DTC advertising in the U.S. often exaggerates benefits while downplaying risks, leading to increased prescriptions for drugs like statins or antidepressants without clear clinical need. For example, a 2019 study found that U.S. patients were twice as likely to request advertised medications compared to their Canadian counterparts, despite similar healthcare systems.
From a practical standpoint, the absence of DTC advertising in most countries fosters a more measured approach to medication use. In Germany, for instance, pharmaceutical companies must adhere to strict guidelines when promoting products to doctors, ensuring that marketing does not overshadow clinical efficacy. This contrasts with the U.S., where ads for drugs like erectile dysfunction treatments or insomnia medications often target broad audiences, sometimes leading to misuse or unnecessary prescriptions. For patients, this means relying on healthcare providers for accurate information rather than persuasive marketing campaigns.
Persuasively, the global trend toward banning DTC advertising underscores a commitment to ethical healthcare practices. Countries like New Zealand and Japan view such ads as a potential threat to public trust in medicine, arguing that profit motives should not drive treatment decisions. By contrast, the U.S. model often prioritizes market share over patient welfare, as evidenced by the $6.58 billion spent on DTC advertising in 2022 alone. This disparity highlights the need for a reevaluation of U.S. policies, particularly as other nations achieve comparable health outcomes without relying on consumer-targeted drug promotions.
In conclusion, the global variation in DTC pharmaceutical advertising reflects differing priorities in healthcare. While the U.S. embraces a market-driven approach, most countries opt for caution, safeguarding patients from potential harms. For individuals navigating this landscape, understanding these differences can empower better decision-making. Whether in the U.S. or abroad, patients should critically evaluate medication information, consult healthcare providers, and prioritize evidence over advertising claims.
Cultural Missteps in Ads: Which Companies Often Miss the Mark?
You may want to see also
Explore related products






![]()
Industry Impact: Advertising boosted drug sales and patient requests for specific medications significantly
The year 1985 marked a pivotal shift in healthcare when the Food and Drug Administration (FDA) relaxed its guidelines, allowing pharmaceutical companies to advertise prescription drugs directly to consumers (DTCA). This move, initially seen as a way to empower patients, unleashed a tidal wave of change. Television screens, magazines, and later the internet became flooded with ads for medications, transforming the doctor-patient dynamic and the pharmaceutical landscape forever.
One immediate and undeniable consequence was a surge in drug sales. Companies strategically targeted specific demographics with tailored campaigns. For instance, ads for cholesterol-lowering statins often featured middle-aged individuals enjoying active lifestyles, subtly suggesting the medication as a key to maintaining vitality. This approach resonated, leading to a significant increase in statin prescriptions, particularly among those who might not have previously been considered high-risk.
The impact extended beyond sales figures. Patients, armed with information from advertisements, began entering doctor's offices with specific medication requests. This shift challenged the traditional model where doctors held sole authority in prescribing decisions. While some argued this empowered patients to take a more active role in their health, critics pointed to the potential for over-medicalization and unnecessary prescriptions driven by persuasive marketing rather than clinical need.
A 2003 study published in the Journal of the American Medical Association found that DTCA was associated with a 16-23% increase in prescriptions for advertised drugs. This raises important questions about the ethical implications of such aggressive marketing. Are patients truly making informed decisions, or are they being swayed by emotionally charged advertisements?
The rise of DTCA also highlights the need for critical thinking and open communication between patients and healthcare providers. Patients should approach drug advertisements with a discerning eye, understanding that these are marketing tools designed to sell products. Discussing the benefits, risks, and alternatives to advertised medications with a doctor is crucial for making informed healthcare choices.
Uncover Advertising Company Secrets: Research Tips for Informed Decisions
You may want to see also
Explore related products






![]()
Ethical Concerns: Critics argue ads prioritize profits over public health and medical necessity
The year 1985 marked a turning point in the pharmaceutical industry when the Food and Drug Administration (FDA) began allowing drug companies to advertise prescription medications directly to consumers. This shift, initially limited to print media, expanded to television and digital platforms in 1997, following the FDA’s issuance of guidelines for direct-to-consumer (DTC) advertising. While proponents argue that these ads empower patients by increasing awareness of treatment options, critics contend that they often prioritize corporate profits over public health and medical necessity. This tension raises ethical concerns about the influence of such advertising on prescribing practices, patient behavior, and healthcare costs.
Consider the case of statins, a class of drugs used to lower cholesterol. Ads for these medications frequently depict active, healthy individuals enjoying life, subtly suggesting that taking the drug will lead to similar outcomes. However, such portrayals often gloss over critical details, such as the fact that statins are most effective for patients with a history of cardiovascular disease or significantly elevated cholesterol levels. For low-risk individuals, the benefits may not outweigh potential side effects like muscle pain or liver damage. Critics argue that these ads encourage overprescription, as they appeal to a broad audience without adequately addressing the specific medical criteria for use. This not only risks unnecessary exposure to medication but also drives up healthcare costs, as patients and insurers bear the financial burden of potentially avoidable prescriptions.
From a persuasive standpoint, the ethical dilemma deepens when examining the psychological tactics employed in pharmaceutical ads. These campaigns often use fear-based messaging, highlighting the dangers of untreated conditions while offering the advertised drug as a simple solution. For instance, ads for osteoporosis medications frequently emphasize the risk of fractures, particularly among older adults. While raising awareness is valuable, such messaging can create anxiety, prompting patients to request medications they may not need. Physicians, in turn, may feel pressured to prescribe these drugs to alleviate patient concerns, even when alternative, non-pharmacological interventions—like dietary changes or physical therapy—could be equally or more effective. This dynamic underscores the concern that DTC advertising manipulates emotions rather than fostering informed decision-making.
A comparative analysis of countries with and without DTC advertising further illuminates its ethical implications. In nations like the United Kingdom and Australia, where such advertising is prohibited, healthcare systems tend to prioritize evidence-based prescribing and cost-effectiveness. Studies show that these countries have lower per capita prescription drug spending compared to the United States, where DTC advertising is pervasive. For example, the U.S. spends nearly twice as much on prescription drugs as other high-income nations, despite similar health outcomes. This disparity suggests that DTC advertising contributes to a culture of overmedication, diverting resources from more critical public health initiatives, such as preventive care and mental health services.
To address these ethical concerns, practical steps can be taken to mitigate the negative impact of pharmaceutical advertising. First, regulatory bodies could mandate the inclusion of more detailed risk information in ads, ensuring that potential side effects and appropriate use criteria are clearly communicated. Second, healthcare providers should proactively educate patients about the limitations of advertised medications, encouraging a shared decision-making process that considers individual health needs. Finally, policymakers could explore alternatives to DTC advertising, such as public health campaigns focused on disease prevention and lifestyle modifications. By shifting the focus from profit-driven marketing to patient-centered care, these measures could help restore balance to the pharmaceutical landscape, ensuring that medical necessity remains the guiding principle in treatment decisions.
Pioneering Brands: The First Companies to Advertise on Snapchat
You may want to see also
Frequently asked questions
The United States began allowing direct-to-consumer (DTC) pharmaceutical advertising in 1985, though it became more widespread and regulated after 1997 when the FDA issued guidelines easing restrictions.
The U.S. allowed pharmaceutical advertising to promote patient awareness of medical conditions and treatment options, encourage conversations between patients and doctors, and increase access to prescription medications.
Yes, but only a few. New Zealand allowed pharmaceutical advertising in 2010, and Canada permits limited advertising for specific medications. Most countries, including those in the EU, still prohibit direct-to-consumer pharmaceutical advertising.
Pharmaceutical advertising has increased awareness of medical conditions but has also been criticized for contributing to higher healthcare costs, overprescription, and the promotion of brand-name drugs over generics.
Yes, pharmaceutical ads must include information about risks and side effects, and they are regulated by the FDA to ensure they are not misleading. However, enforcement of these rules varies.






















